





The pain started in your lower back. Then it moved into your glute. Now it shoots down the back of your leg when you stand up from your desk or step off a curb. Maybe it’s a burning line from your hip to your calf. Maybe it’s numbness in your foot that comes and goes. You’ve been stretching, icing, taking ibuprofen, and sleeping with a pillow between your knees for weeks. It gets a little better, then comes right back. If you’re searching for answers at this point, you’ve probably already come across the word sciatica, and you’re wondering whether a Manhattan chiropractor can actually help or whether you’re headed for surgery. The answer depends entirely on what’s causing the nerve irritation, and that’s the part most people skip.
Sciatica Is a Symptom, Not a Diagnosis
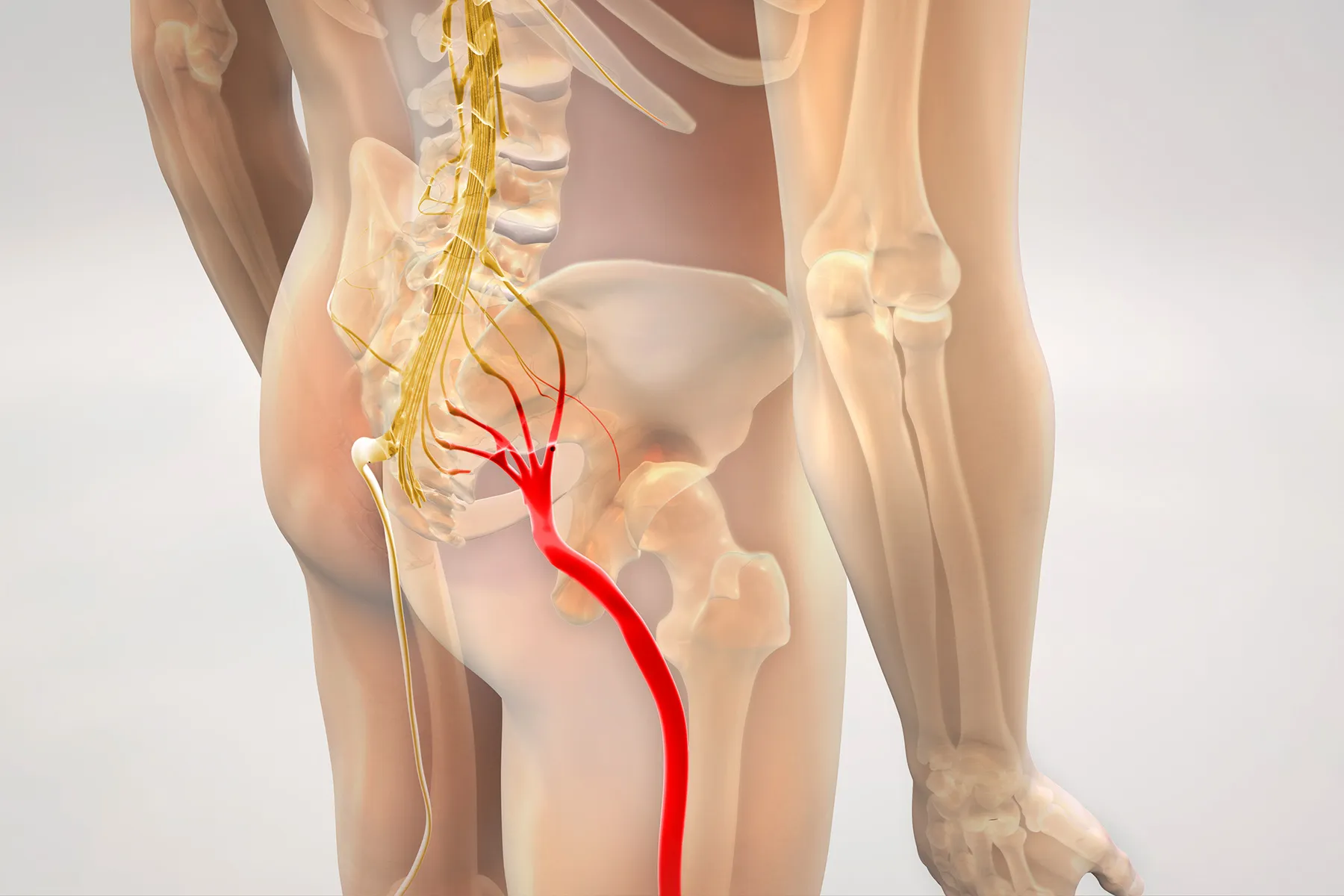
This is the most important thing to understand, and it’s where a lot of people get stuck. Sciatica describes a pattern of pain that follows the sciatic nerve from the lower back through the buttock and down the leg. It tells you which nerve is irritated. It doesn’t tell you why.
Three different conditions produce sciatic nerve pain, and each one requires a different treatment approach. Treating the wrong cause is the main reason sciatica “won’t go away” for people who’ve been managing it on their own or receiving generic treatment.
Disc Herniation
A herniated disc in the lumbar spine, most commonly at L4-L5 or L5-S1, is the cause most people think of first. The disc’s soft inner material pushes through the outer wall and presses on the nerve root as it exits the spinal column. The pain is often sharp, electrical, and worsened by sitting, bending forward, or coughing. It frequently comes on after a specific incident: lifting something heavy, twisting awkwardly, or a sudden load on a spine that was already degenerating.
Disc herniations vary in severity. A small protrusion may irritate the nerve intermittently. A larger extrusion can cause constant pain, significant leg weakness, or changes in bladder and bowel function (which is a medical emergency requiring immediate evaluation, not chiropractic care). Most disc herniations fall somewhere in the mild to moderate range and respond well to conservative treatment if the right approach is applied early.
Piriformis Syndrome
The piriformis is a small muscle deep in the buttock that runs from the sacrum to the top of the femur. The sciatic nerve passes directly beneath it in most people, and in about 15 to 20 percent of the population, the nerve actually passes through the muscle itself. When the piriformis tightens, spasms, or becomes inflamed, it compresses the sciatic nerve and produces pain that mimics a disc herniation.
The key difference: piriformis syndrome typically doesn’t produce significant lower back pain. The pain concentrates in the buttock and runs down the leg, and it’s often aggravated by prolonged sitting (particularly on hard surfaces), crossing the legs, or climbing stairs. People who sit on a wallet in their back pocket for hours, or who sit on the subway during a long commute, are classic piriformis syndrome candidates.
This distinction matters because the treatment for piriformis syndrome targets the muscle, not the spine. Spinal adjustments alone won’t resolve piriformis compression. The muscle needs direct soft tissue work, stretching, and often strengthening of surrounding hip stabilizers to prevent recurrence.
Spinal Stenosis
Spinal stenosis is a narrowing of the spinal canal or the neural foramen (the openings where nerves exit the spine). It’s more common in patients over 50 and develops gradually as the spine degenerates. The narrowing compresses nerve roots and produces sciatic symptoms that are typically worse with standing and walking and better with sitting or bending forward.
That positional pattern is the hallmark. If your leg pain gets worse the longer you stand or walk and improves when you sit down or lean on a shopping cart, stenosis is the likely culprit. It’s the opposite pattern of disc herniation, where sitting usually makes things worse.
Stenosis responds to specific types of chiropractic care and physical therapy, particularly flexion-based exercises and decompression techniques that open the narrowed spaces. Extension-based treatments that work well for disc patients can actually aggravate stenosis, which is another reason why identifying the correct cause before starting treatment is critical.
Why Generic Treatment Fails
Most people with sciatica start with the same approach regardless of the cause: rest, ice, anti-inflammatory medication, and generic stretching. This works sometimes, by coincidence, when the cause happens to be mild and the body’s own healing resolves it within a few weeks.
When it doesn’t work, people escalate to the next level of generic care: a cortisone injection into the lumbar spine. Epidural steroid injections can provide temporary relief by reducing inflammation around a compressed nerve root. But if the compression is coming from the piriformis muscle rather than a disc, injecting the spine misses the source entirely. The pain returns because the injection treated the wrong location.
This is the cycle that leads people to search “sciatica won’t go away” at 11 p.m. They’ve done the stretches. They’ve taken the medication. Maybe they’ve had an injection. Nothing has produced lasting relief because nobody identified which of the three causes is driving their specific symptoms.
How a Manhattan Chiropractor Evaluates Sciatica
At I Know My Chiro, Dr. Casanova’s evaluation of a sciatica patient starts with a detailed history: when the pain started, what makes it worse, what makes it better, whether there was a specific triggering event, and where exactly the pain travels. These details narrow the likely cause before any physical testing begins.
Orthopedic and neurological testing follows. Specific tests differentiate between disc, piriformis, and stenosis as the source of compression. A straight leg raise that reproduces leg pain at a low angle suggests disc involvement. Pain with resisted external rotation of the hip points to the piriformis. Symptoms that worsen with lumbar extension and improve with flexion suggest stenosis.
The treatment plan is built around the findings. For disc-related sciatica, spinal adjustments focus on restoring segmental mobility in the lumbar spine, reducing pressure on the affected nerve root, and creating the mechanical environment for the disc to heal. Flexion-distraction technique, a gentle form of spinal decompression performed on a specialized table, is particularly effective for disc patients.
For piriformis syndrome, the approach shifts to targeted soft tissue work on the piriformis and surrounding hip rotators, combined with specific stretching and hip stabilization exercises. Chiropractic adjustment of the sacroiliac joint is often part of the treatment because SI joint dysfunction frequently contributes to piriformis tightening.
For stenosis, treatment emphasizes flexion-based mobilization, core stabilization, and activity modification to manage symptoms within the structural limitations of the narrowed canal.
In all three cases, physical therapy and rehabilitation exercises play a role in preventing recurrence. The adjustment addresses the immediate mechanical problem. The rehab work makes the correction durable.
When Sciatica Requires More Than Chiropractic Care
Not every case of sciatica is appropriate for chiropractic management. Progressive leg weakness, loss of sensation in the foot, or any change in bladder or bowel function are signs of severe nerve compression that may require surgical evaluation. A responsible chiropractor screens for these red flags at every visit and refers promptly when the clinical picture warrants it.
For the majority of sciatica patients, those with moderate pain and functional limitation but no neurological emergency, chiropractic care combined with physical therapy produces outcomes that are comparable to more invasive interventions with significantly less risk and downtime. The key is getting the cause right first.



